


ADVERTISEMENT
Development of a Content-Validated Venous Ulcer Guideline
Venous ulcers (VU) profoundly decrease a person’s quality of life.1,2 They affect up to 1% of the population over 60 years of age at any given time3,4 and cost an estimated $2.5 to $3.5 billion US healthcare dollars annually.5 A MEDLINE literature search revealed that VU patients currently experience an evidence-reimbursement gap for compression modalities and patient education essential for effective, cost-effective VU healing outcomes.6 To lay the foundation for closing this gap, the Association for the Advancement of Wound Care (AAWC) Government and Regulatory Task Force (henceforth abbreviated “the Task Force”) resolved to develop a content-validated VU guideline based on objective summaries of best available evidence supporting each step of VU care.
Methods
The multidisciplinary, all-volunteer Task Force including 11 Advanced Practice Nurses or Wound Ostomy Continence Nurses (WOCNs), five physicians, four physical therapists, two PhDs, one Doctor of Podiatric Medicine, and a Registered Pharmacist first met on April 29, 2002, at the Symposium for Advanced Wound Care in Baltimore, Md. The Task Force adopted the mission of helping US government and regulatory authorities close gaps between wound care evidence and practice. The Task Force used Total Quality Leadership7 tools including brainstorming and fishbone diagrams to identify regulatory and reimbursement issues preventing professionals from practicing quality evidence-based VU care. They developed and prioritized strategies for resolving these issues to help close the gap between VU evidence-based care and actual practice.
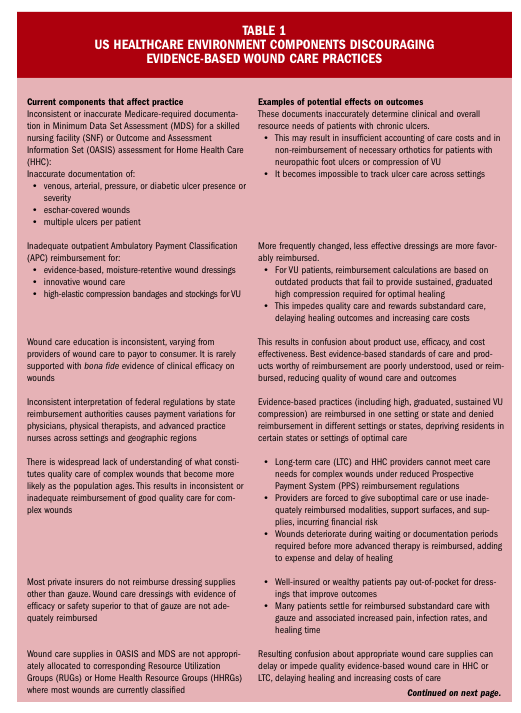
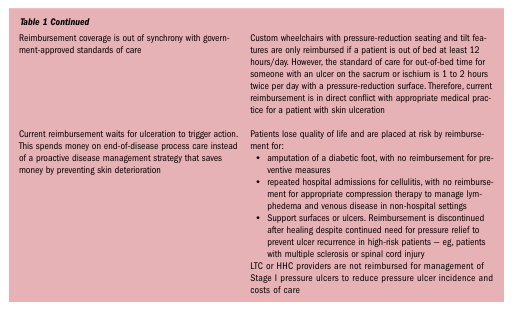
The Task Force identified eight issues impeding evidence-based, cost-effective VU practice (see Table 1) and resolved to outline the best available evidence supporting each step in VU care. Steps were listed from published algorithms and best evidence supporting each step of care was included to create an evidence-based decision tool for care providers and reimbursement authorities. In addition to including outcome evidence for each step, the Task Force additionally intended to include the reimbursement status of the step to help authorities define and reduce gaps between evidence-based practice and reimbursement policies. However, reimbursement policies are so varied across settings, professions, states, and regions that reimbursement listings proved impractical. In the end, the Task Force focused on generating an inclusive algorithm annotated with the best available research, hoping to set the stage for reimbursing high quality, evidence-based, cost-effective wound care practice in patients with venous disease.
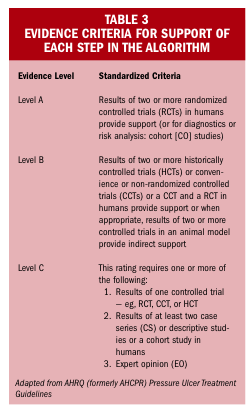
Algorithm development. The steps to algorithm development are summarized in Table 2. The Task Force created a composite of all steps in all algorithms for venous ulcer management based on guidelines, consensus statements, critical pathways, and standards published before August 20023,8-21; this was called the Venous Ulcer Care Initiative (VUCI) algorithm. Next, individual members with experience in each aspect of care searched the literature using MEDLINE, CINAHL, and EMBASE databases to identify and list up to five of the best evidence level references supporting that aspect. Quality of evidence was assessed according to the criteria in Table 3, adapted from prior AHRQ guidelines for pressure ulcer care.22,23 The resulting guideline was neither a consensus-based document nor a comprehensive or systematic review of all literature supporting each aspect of care. Rather, it was a compendium of objectively rated best currently available evidence that the Task Force could find supporting VU care identified in the combined VU algorithms compiled from the literature. It was intended for use as a continuously improving framework within which to evaluate reimbursement status in light of the evidence supporting each element of VU care and to identify research and reimbursement gaps supporting VU clinical practice.

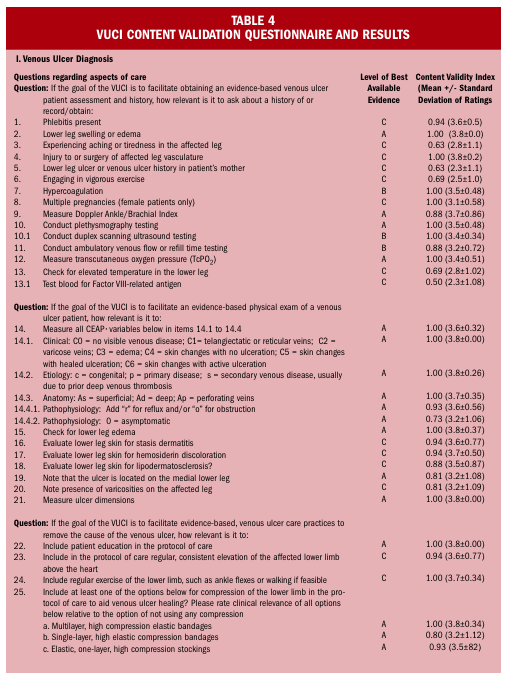
Content validity testing. Establishing validity is crucial for any instrument that affects patient care decisions.18 The VUCI consisted of 76 aspects of VU care divided into six areas, including diagnosis, alleviating the cause of ulceration, providing local care, care modalities if conservative treatment fails to improve outcomes, surgical options to use if conservative treatment fails, and continuing care until healing or to prevent recurrence. Many of these aspects of care had not undergone content validity testing in prior literature.
To establish content validity of each item of the VUCI Algorithm, the judgment quantification process was used18,24 by a multidisciplinary convenience sample of volunteer wound care professional respondents from among the 2004 AAWC Board of Directors and the Research, Quality of Care, and Government & Regulatory Task Forces. The Content Validity Index (CVI) was calculated as the percent of respondents rating the clinical relevance or validity of each item as 3 or 4 using a 4-point Likert scale where 1 = not relevant, 2 = unable to assess relevance without further information, 3 = relevant but needs minor attention, and 4 = very relevant and succinct.
Reimbursement survey. After completing and validating the algorithm, the Task Force conducted a reimbursement survey distributed by email to 1,514 AAWC members via email in June 2004 to see if the original issues had changed or reimbursement had improved. The eight returned surveys and associated comments were analyzed.
Data analysis and statistical methods. Content validity data from respondents were entered into an EXCEL® (Microsoft, Seattle, Wash) database and analyzed using the program’s automatic functions for descriptive statistics. Mean content validity score and the proportion of respondents rating each item a 3 or 4 (CVI) were calculated for each of the aspects of care. A VUCI item remained in the final algorithm, now a content-validated guideline, if it was supported by A-level evidence, if it had a CVI of 0.75 or more, or if it met both criteria. Reimbursement survey responses were analyzed quantitatively (EXCEL database and descriptive statistics) and qualitatively by grouping written responses into thematic categories.
Results
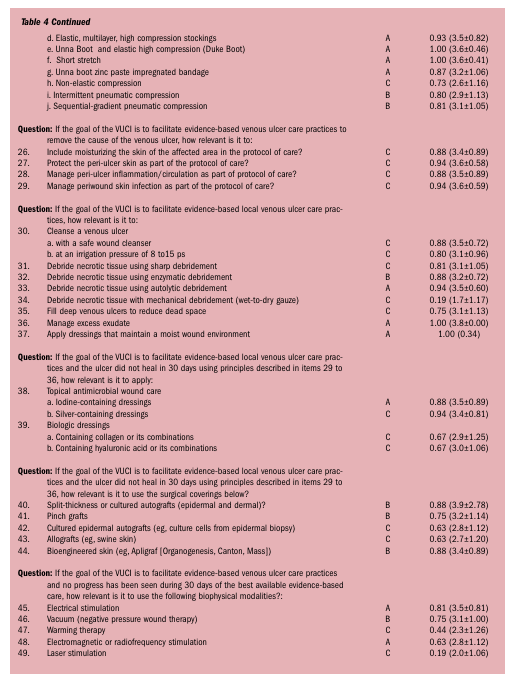
Content validation. Sixteen wound care professionals participated voluntarily in the content validation exercise including one physician, seven WOCNs (three of which were doctorally prepared), three advanced practice nurses, four physical therapists, and one PhD. Several participants engaged in both wound care practice and education or practiced in multiple settings. Respondents had an average of 3.2 (SD = 1.0) years of wound care practice. Of the wounds they treated, 32% were venous ulcers, 31% were pressure ulcers, and 11% were diabetic foot ulcers. Three participants spent an average of 43% of their time in acute care inpatient management. One practiced full time in an acute care outpatient facility. Three spent an average of 40% of their time in an extended care setting and three practiced solely in a skilled nursing facility. Five spent an average of 31% of their time in home care. One spent 20% of the time in acute care. Two spent an average of 60% of their time in a separate wound clinic. The physician practiced in acute care and office settings. Two respondents were in government or educational institutions. The items compiled from existing algorithms, level of best available evidence for each item, and corresponding CVI values + standard deviation from the content validation study are presented in Table 4. Items with a CVI >0.75 supported by B- or C-level research present opportunities for further study. For example, items for exercise and elevation of the lower leg above the heart, moisturizing, and protecting or managing periwound inflammation or infection had opinion-based content validity indices >0.75 without the support of A-level controlled clinical studies. Controlled studies are also needed to support venous ulcer cleansing and debridement, filling dead space, and use of silver dressings.
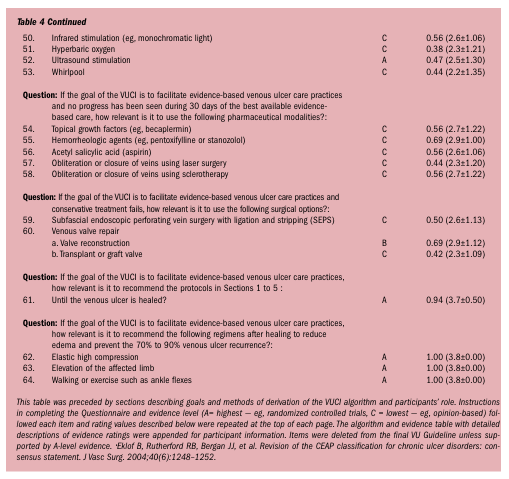
The resulting AAWC VU Guideline containing items with A-level best evidence plus those with a CVI of 0.75 or more was accepted by the Agency for Healthcare Research and Quality National Guideline Clearinghouse and can be viewed or downloaded free of charge at https://www.guideline.gov or at the AAWC website https://www.aawcone.org.
All 16 respondents believed that a team approach is required for optimal VU management. Most commonly team member suggestions were from a physician, nurse or specialty nurse, physical therapist, and vascular specialist. All believed that evidence-based VU practice would speed healing. Of the respondents, 81% believed evidence-based VU care would reduce the costs of VU care in their environment, 56% felt that it may increase costs now but decrease them in the long run, and 19% believed that it would increase care costs indefinitely. Of the 16 respondents, 10 believed the most important advantages of an evidence-based approach to VU care would be a systematic and organized approach to treatment, guidelines for novice wound care clinicians, and better outcomes for patients with more satisfied patients, payors, and wound care clinicians. Most respondents listed inadequate reimbursement and difficulty evaluating or finding evidence as disadvantages of evidence-based VU care.
As an independent check on the content validation VU practice data, Caroline Fife, MD, provided an analysis of the US-based Intellicure Clinical Documentation and Facility Management Software (ICDFMS) database25 containing 622 VU patients with 1,377 VU for a perspective of VU practice in the US. Approximately one third of identifiable VUs in this database did not receive compression of any sort. The most common form of compression used was a four-layer bandage (21%), followed by double-layer elastic tubular bandage (18%), compression stockings (9%), or short-stretch compression (4%).
Reimbursement survey. The 2005 Reimbursement Survey was returned by eight clinicians: two physicians, three physical therapists, one advanced practice nurse/CWOCN, one RN, and one anonymous respondent, together experiencing a total of 10,000 patient visits per year for wound care. Aspects of practice supported by A-level best evidence with inadequate reimbursement or reimbursement that had been refused based on respondent experience included patient education and elastic compression bandages as well as stockings needed both to heal venous ulcers and to prevent their recurrence.
Venous ulcer patients remained in their professional care for an average of 14 (8 to 30) weeks and were seen once or twice per week. Compression was performed on 94% of visits, requiring an average of 16 minutes per visit. Venous ulcer evaluation (eg, measuring wound dimensions or percent or area of necrotic tissue) was performed during 67% of visits, taking an average of 13 (2 to 45) minutes per initial visit and 6 (2 to 15) minutes on later visits. Management (eg, cleansing or topical care) was performed during 92% of visits with initial visits taking an average of 11 (4 to 20) minutes and later visits taking 9 (4 to 15) minutes. Debridement was performed during 46% of visits, taking an average of 12 (4 to 20) minutes per initial visit or 7 (0 to 20) minutes on later visits. Compression, performed on an average of 94% of visits, took an average of 16 (7 to 30) minutes on the first visit and 20 (5 to 60) minutes on later visits. Percent of procedural or supply costs billed separately varied between 0% and 100% for all aspects of care, as did percents of billing normally paid. Procedural payment by different payors was reported to differ. Respondents emphasized that VU patients are never cured and that once healed, a VU patient requires graduated compression of the lower leg adequate to aid venous return for the rest of his or her life.
Survey respondents and Task Force members reported that their facilities were cited and forced to pay fines for using evidence-based sustained, graduated, high elastic compression modalities to manage VU patients because they coded these procedures with the only existing Common Procedural Terminology (CPT) code for compression, CPT 29580. Reimbursement varied widely among payors and was usually insufficient for and/or inconsistent with evidence-based VU care. Supplies were generally not reimbursed, placing the economic burden of VU care on the provider and/or patient. Four of the five respondents who provided comments said they may have to close their facility due to lost revenue while providing high quality evidence-based VU care. One of these four has now closed its leg ulcer clinic.
Scenarios (see Appendix I) were written by qualified wound care professionals in relevant settings of care to illustrate the reimbursement inadequacy of items in the algorithm typically used for VU care. These example scenarios illustrate the impact of current reimbursement methodologies on real-world care. They may or may not match the reader’s experience due to expense and reimbursement variability according to setting and location of service, professional specialist delivering the care, type of relative value unit (RVU), complexity of service (Evaluation and Management codes), code modifiers such as unintended additional assessment or care, and procedural codes and diagnoses attached to such codes.
Discussion
This research established a content-validated VU algorithm supported by best available evidence that met US Department of Health and Human Services AHRQ criteria for acceptance as a venous ulcer guideline. Other content-validated algorithms have been published for general wound care21,26 and for nursing education to prevent pressure ulcers.27 To the authors’ knowledge, this is the first formally content-validated VU guideline in the literature. This guideline will be updated every 2 years to incorporate new evidence, offering a benchmark for professional VU care and reimbursement.
The reimbursement survey findings and low incidence of compression use on VU patients in the independent analysis of the ICDFMS database reflect a disturbing trend in US healthcare. By limiting reimbursement of care based on the best available evidence, reimbursement authorities may be unintentionally limiting economic access to quality wound care.28 The AAWC Survey and the real wound care scenarios illustrate how government and private reimbursement policies are short-changing patients with venous disease as well as those trying to provide these patients with high quality care. Substandard care has the potential to delay healing and increase the risk of poor outcomes. This increases the economic, clinical, and humanistic burdens of chronic wound care at a time when the elderly population at risk of chronic wounds is growing, along with the US budget deficit. If the current reimbursement system’s stated goal is to improve the quality of care,29 now is the time to do so before spiraling costs of caring for chronic wounds consume the resources that should be spent healing and preventing them.
The content-validated AAWC VU Guideline and its associated Evidence Table have been placed on the National Guideline Clearinghouse and AAWC websites to enable use by professionals managing VU patients and to encourage appropriate reimbursement of VU practice based on the best evidence the Task Force could find at the time of the literature search.
This project identified several opportunities for future research. Items with high content validity and C-level evidence signal the need for controlled clinical research in the areas of leg elevation or exercise, management of venous ulcer periwound skin, necrotic tissue, and inflammation or infection.
Limitations
A limitation of this guideline is that some steps lack Level A support. Content validation is a powerful tool for quantifying expert opinion consensus but it is not a substitute for prospective, randomized controlled studies of safety or efficacy of each aspect of VU care. The evidence supporting each aspect of care will improve as Level A studies are conducted for those steps currently lacking sufficient evidence to qualify for Level A support. The steps with B or C level evidence suggest future research focused on areas of venous ulcer practice needing a more respectable research base.
Another limitation is the sample size and potential response bias of respondents to the Reimbursement Survey. Less than 1% of the AAWC members receiving the survey completed and returned it. Despite the limited number of respondents, these clinicians represented care delivered to a significant number of patients. At the time of the survey (2004), reimbursement was an emerging concern among clinicians, many not even aware of clinical impact. Over the subsequent 2 years, this issue has moved to the forefront and reimbursement has surfaced as a powerful factor limiting care decisions.
As the multidisciplinary Task Force, comprised of members of a variety of specialist physician, nursing and physical therapist societies, worked together to compile and validate this evidence-based algorithm, they realized the value each professional brings to VU patient care and the power with which reimbursement can encourage or discourage quality care. The Task Force recommended developing a recognized wound care subspecialty that links reimbursement to expertise—eg, a subspecialty in venous ulcer care for experts who know and practice evidence-based management of patients with venous disorders. Before this can happen, wound care professionals would need to agree on objectively standardized, reliable, validated documentation and patient-centered, evidence-based protocols of care. This requires rigorous operational definitions for procedures and consensus on care across disciplines. Professional societies and government agencies would need to speak with one voice, sharing a unified, coordinated approach to deliver and reimburse quality wound care. The Task Force offers the AAWC VU Guideline as a first step toward unifying venous ulcer care supported by adequate reimbursement.
The authors plan to update the Guideline annually with new evidence and successive review and validation by other societies so it can continually improve as a multidisciplinary resource for professionals and payors serving patients with venous disorders. While availability of a guideline based on best available evidence is a step toward improving the quality of venous ulcer care, US clinics continue to lose revenue if they provide optimal care for venous ulcers. Without improvements in reimbursement of evidence-based venous ulcer care, patients, providers, and payors will continue to pay the price of suboptimal VU practices.
Conclusion
The AAWC Government and Regulatory Task Force established a content-validated venous ulcer guideline supported with a summary of best available evidence for each element of VU practice. This dynamic document is a first step toward aligning the language, practice, and reimbursement of venous ulcer care.
This research was conducted by volunteers on the Government and Regulatory Task Force (G&R Task Force) of the Association for the Advancement of Wound Care (AAWC), which provided meeting and teleconference support and funds for obtaining reprints of articles during the period of the AAWC Venous Ulcer Guideline development.
Disclosures: Dr. Bolton is a stockholder and former employee of ConvaTec, A Bristol-Myers Squibb Company, Princeton, NJ, and Johnson & Johnson, Somerville, NJ. Ms. Dotson is a former employee of ConvaTec. Mr. Laraus is a Clinical Consultant for Davol, Inc., Cranston, RI. Dr. Phillips is a consultant to ConvaTec and Smith & Nephew. Dr. Patterson has received speaker honoraria and/or research grants and/or served as a consultant, paid advisory board member, and/or expert witness for KCI, Smith & Nephew, Novartis, Johnson & Johnson Wound Management, Celleration, and/or Argentum Medical.
Acknowledgements
The Task Force acknowledges Robert Kirsner, MD, whose leadership as President of the AAWC Board of Directors during 2001–2003 made this project possible; and the AAWC staff, Tina Thomas and Cathy DiJohn, who respectively aided in communications and in entering the content validation data. The authors especially thank the additional volunteer content validation respondents: M. Armstrong, RN, MSc, CWOCN; M. Cooper, RN, CWOCN, DNC; R. Cordrey, PT, PhD candidate, MSPT, MPH, CWS; C. Hawkins, RN, BSN, CWOCN; J. Jones, BSN, RN, ET, CWOCN; D. Krasner, PhD, MS, RN, CWOCN, CWS, FAAN; S. Lee, MPT, CWS; C. Milne, APRN, MSN, CWOCN; P. Scarborough, PT, MS, CDE, CWS; and Task Force members who helped to make this project multidisciplinary, fair, balanced, and evidence-based: S. Alter, DPM; A. Batzler, MN, FNP; N.R. Bruno, RN, BSN, ET; G. Chudleigh, MS, PT, CWS; P. Erwin-Toth, RN, MSN, CWOCN; G. Everhart, DPT; R.S. Jordan, RN, BSN, CWOCN; S.K. Lee, MD, FACS; C.H. Lyder, ND, APRN, CS, GNP; T. Mulloy, BSN, RN, ET; M. Nusgart, RPh; L. Dahl Popkes, RN, CWOCN; S. Sinkovic Girolami, RN, BSN, CWOCN; and M. Southworth, MD. 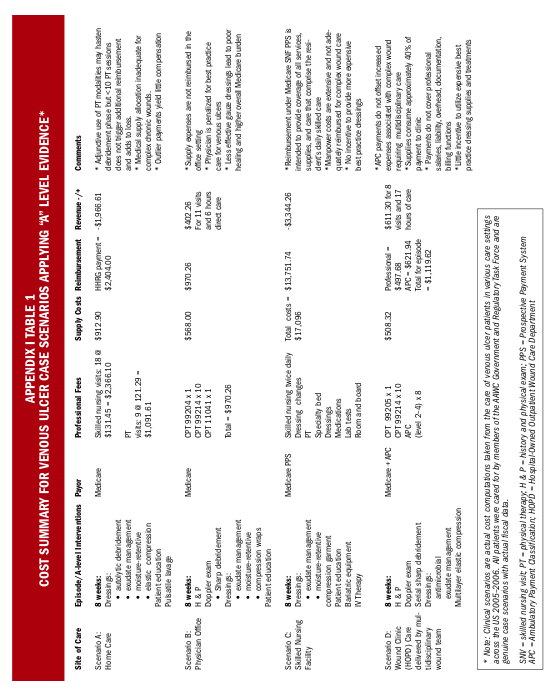



1. Phillips T, Stanton B, Provan A, Lew R. A study of the impact of leg ulcers on quality of life: financial, social and psychological implications. J Am Acad Dermatol. 1994;31:49–53.
2. Abbade LP, Lastoria S. Venous ulcer: epidemiology, physiopathology, diagnosis and treatment. Int J Dermatol. 2005;44(6):449–456.
3. Heit JA, Rooke TW, Silverstein MD, et al. Trends in the incidence of venous stasis syndrome and venous ulcer: a 25-year population-based study. J Vasc Surg. 2001;33:1022–1027.
4. Cornwall JV, Dore CJ, Lewis JD. Leg ulcers: epidemiology and aetiology. Br J Surg. 1986;73:693–696.
5. McGuckin M, Kerstein M. Venous ulcers and family physicians. Adv Skin Wound Care. 1998;11:344–346.
6. Korn P, Patel ST, Heller JA, et al. Why insurers should reimburse for compression stockings in patients with chronic venous stasis. J Vasc Surg. 2002;35(5):950–957.
7. Hourani LL, Hurtado SL. Total quality leadership in the US Navy: effective for health promotion activities? Prev Med. 2000;30(6):478–484.
8. Alguire PC, Mathes BM. Chronic venous insufficiency and venous ulceration. J Gen Internal Med. 1997;12:374–383.
9. Alexanderhouse Group. Consensus paper on venous leg ulcers. Phlebol. 1992;7:48–58.
10. Black SR. Venous stasis ulcers: a review. Ostomy Wound Manage. 1995;41(8):20–29.
11. Burton CS. Venous ulcers. Amer J Surg. 1994;167(suppl 1A):37S–39S.
12. Cherry GW, Cameron J, Ryan TJ. Blueprint for the treatment of leg ulcers and the prevention of recurrence. WOUNDS. 1993;3:2–5.
13. Falanga V. Venous ulceration: assessment, classification and management. In: Krasner D, Kane D. Chronic Wound Care, 2nd ed. Wayne, Pa: Health Management Publications, Inc;1997:165–171.
14. Kerstein MD. The non-healing leg ulcer: peripheral vascular disease, chronic venous insufficiency and ischemic vasculitis. Ostomy Wound Manage. 1996;42(10 suppl A):19S–35S.
15. McGuckin M, Waterman R, Brooks J, et al. Validation of venous leg ulcer guidelines in the United States and United Kingdom. Amer J Surg. 2002;183:132–137.
16. Nelson EA, Dale J. The management of leg ulcers. J Wound Care. 1996;5(2):73–76.
17. Morrison M, Moffatt C, Bridel-Nixon J, Bale S. Leg ulcers. In: Morrison M, et al. Color Guide to the Nursing Management of Chronic Wounds. 2nd Ed. London, UK: Mosby;1997:177–220.
18. Phillips T. Successful methods of treating leg ulcers. Postgrad Med. 1999;105(5):159–180.
19. Royal College of Nursing. The management of patients with venous leg ulcers: Clinical Practice Guideline. 1998; The RCN Institute, Center for Evidence-based Nursing, University of York and School of Nursing, Midwifery and Health Visiting, University of Manchester. Available at: www.rcn.org.uk/resources/guidelines. Accessed October 24, 2006.
20. Stacey M, Falanga V, Marston W, et al. The use of compression therapy in the treatment of venous leg ulcers: a recommended management pathway. EWMA J. 2002;2(1):3–7.
21. Beitz J, van Rijswijk L. Using wound care algorithms: a content validation study. JWOCN. 1999;26:238–249.
22. Panel for the Prediction and Prevention of Pressure Ulcers in Adults. Pressure Ulcers in Adults: Prediction and Prevention. Clinical Practice Guideline, Number 3. AHCPR Publication No. 92-0047. Rockville, Md: US Department of Health and Human Services;1992.
23. Bergstrom N, Bennett MA, Carlson CE, et al. Pressure Ulcer Treatment. Clinical Practice Guideline, Number 15. AHCPR Publication No. 95-0653. Rockville, Md: US Department of Health and Human Services;1992.
24. Yaghmaie F. Content validity and its estimation. J Med Education. Spring 2003. Available at: http://www.sbmu.ac.ir/Journal/MedEdu/jm. Accessed September 2, 2003.
25. Fife C. First pass analysis of the Intellicure Clinical Documentation and Facility Management Software (ICDFMS). E-mail communication to L. Bolton. July 25, 2006.
26. Bolton L, McNees P, van Rijswijk L, et al. Wound healing outcomes using standardized care. JWOCN. 2004;31(3):65–71.
27. Sinclair I, Berwiczonek II, Thurston N, et al. Evaluation of an evidence-based education program for pressure ulcer prevention. JWOCN. 2004;31(1):43–50.
28. Eaton MK. The influence of a change in Medicare reimbursement on the effectiveness of Stage III or greater decubitus ulcer home health nursing care. Policy Politics Nurs Pract. 2005;6(1):39–50.
29. Rewarding superior quality care: the Premier Hospital quality incentive demonstration. Centers for Medicare and Medicaid Services Fact Sheet. Updated January 2006. Available at: http://www.cms.hhs.gov/HospitalQualityInits/. Accessed March 21, 2006.




