


ADVERTISEMENT
Treatment of a diabetic hallux ulcer with ultraportable negative pressure wound therapy: a case study
Seton Medical Center - San Francisco Center for Advanced Wound Care Daly City, CA The increasing incidence of diabetes throughout the world will result in a correlational increase in diabetic sequelae such as diabetic foot ulceration.1 Approximately 20.8 million Americans currently live with diabetes and an estimated 333 million adults will be diagnosed by 2025.1 Substantial evidence has been published supporting the use of negative pressure wound therapy (NPWT) as a safe and effective adjunctive modality in the treatment of diabetic foot ulcers (DFUs), including several prospective randomized controlled trials.2-5  One of the more common and complex locations for DFUs is the plantar surface of the toe.6 Use of NPWT for the treatment of wounds in this location traditionally has been challenging, in part due to the small diameter of these wounds. Creating and maintaining an airtight seal in this anatomic location can further be complicated by the wound’s proximity to joints, which inherently have curved surfaces that intermittently move. Traditional NPWT devices that utilize electric pumps may not be ideally suited for these types of smaller-sized wounds due to the configuration of the dressings and size of the pumps. The SNaP® Wound Care System (Spiracur, Sunnyvale, CA), an ultraportable nonelectrically powered NPWT device, has indications and contraindications for use similar to electrically powered systems — ie, removal of small amounts of exudate from chronic, acute, traumatic, subacute, and dehisced wounds, ulcers (such as diabetic or pressure), and surgically closed incisions. This NPWT system utilizes a specialized hydrocolloid dressing, which affords improved flexibility to achieve an airtight seal for challenging anatomical locations, as well as a <3-oz portable, disposable, spring-loaded negative pressure delivery system. These components are specifically designed for smaller wound sizes and facilitate use in challenging anatomical locations such as the plantar toe.
One of the more common and complex locations for DFUs is the plantar surface of the toe.6 Use of NPWT for the treatment of wounds in this location traditionally has been challenging, in part due to the small diameter of these wounds. Creating and maintaining an airtight seal in this anatomic location can further be complicated by the wound’s proximity to joints, which inherently have curved surfaces that intermittently move. Traditional NPWT devices that utilize electric pumps may not be ideally suited for these types of smaller-sized wounds due to the configuration of the dressings and size of the pumps. The SNaP® Wound Care System (Spiracur, Sunnyvale, CA), an ultraportable nonelectrically powered NPWT device, has indications and contraindications for use similar to electrically powered systems — ie, removal of small amounts of exudate from chronic, acute, traumatic, subacute, and dehisced wounds, ulcers (such as diabetic or pressure), and surgically closed incisions. This NPWT system utilizes a specialized hydrocolloid dressing, which affords improved flexibility to achieve an airtight seal for challenging anatomical locations, as well as a <3-oz portable, disposable, spring-loaded negative pressure delivery system. These components are specifically designed for smaller wound sizes and facilitate use in challenging anatomical locations such as the plantar toe. 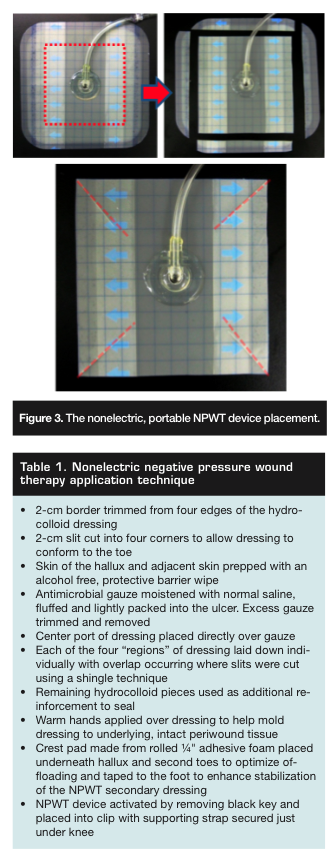 Head-to-head randomized controlled trial data for chronic lower extremity wounds between this device and the electrically powered V.A.C.® Therapy device (KCI, San Antonio, TX) demonstrate no differences in wound healing outcomes or complications.7 In addition, several other studies8-11 have shown that the SNaP device can be both effective and cost-effective in treating diabetic wounds.
Head-to-head randomized controlled trial data for chronic lower extremity wounds between this device and the electrically powered V.A.C.® Therapy device (KCI, San Antonio, TX) demonstrate no differences in wound healing outcomes or complications.7 In addition, several other studies8-11 have shown that the SNaP device can be both effective and cost-effective in treating diabetic wounds.
Case Report
Presentation and assessment. Mr. H is a 52-year-old man with a 10-year history of diabetes mellitus. He arrived in the emergency room (ER) with the onset of fever and chills within a 24-hour period. His medical history and physical revealed an ulcer on his left hallux that had been present for 9 months. He reported the ulcer first appeared as a blister from a pair of tight-fitting shoes. Previous treatments included daily silver sulfadiazine dressing changes and weekly debridements. He reported the ulcer had extended to bone for approximately 3 months. He stopped his doctor visits when he lost his insurance 3 weeks before this ER visit. Testing revealed Mr. H had a white count of 13,200/µL and a left shift. He had a sedimentation rate of 55 mm/hour. A lower extremity ultrasound ruled out deep vein thrombosis (DVT). On exam, his vascular status was intact but his protective sensation bilaterally was absent to the ankles. The left hallux ulcer had thick overlying hyperkeratotic tissue and purulent drainage. There was significant edema of the hallux with mild erythema without warmth.  Treatment. Mr. H was treated overnight in the ER with vancomycin HCl and piperacillin/tazobactam. His wound cultures grew light growth methicillin-sensitive Staphylococcus aureus (MSSA), rare growth Morganella morganii, and rare growth Bacteroides fragilis. One of two blood cultures done in the ER were positive for B. fragilis. An MRI was performed that revealed a small focal osteomyelitis at the distal tuft of the distal phalanx of the hallux. An aggressive excisional bedside debridement of the ulcer and bone was performed with a #15 blade scalpel, forceps, and rongeur in the ER. The remaining bone was firm to touch. After debridement, the ulcer measured 13 mm x 10 mm x 21 mm (length x width x depth) and probed to the distal phalanx of the hallux. Mr. H was discharged from the ER to home with wet-to-moist packing strip dressing changes three times a day and oral levofloxacin (500 mg) daily. He was further instructed to be nonweightbearing. Nine days after his initial presentation into the ER, Mr. H was seen for follow-up at the wound care center. His ulcer post-debridement measured 8 mm x 9 mm x 20 mm (length x width x depth) and continued to probe to firm bone (see Figure 1). He was started on the portable, nonelectrically powered NPWT system, continued on levofloxacin, and allowed to be weight-bearing in a postoperative shoe with a crest pad under the hallux and second toe to offload the ulcer (see Figure 2). The NPWT placement technique is described in Figure 3 and Table 1. After 4 weeks of treatment with the NPWT device, the oral antibiotic was discontinued per recommendation of an infectious disease consult. At week 5 (see Figure 4), NPWT was discontinued due to the small size of wound and Apligraf (Organogenesis, Canton, MA) was applied, followed by Mepitel nonadherent dressing (Mölnlycke, Switzerland) and Contreet foam (Coloplast, Denmark). Mr. H continued to use a postoperative shoe and crest pad. At follow-up 1 week post-Apligraf application, the ulcer was completely epithelialized. Mr. H was followed for an additional 2 months at increasing intervals and the ulcer remained healed (see Figure 5). Prognosis. Mr. H was extremely satisfied with the NPWT treatment. He reported the device did not interfere with his normal daily activities, was never noticed in social situations, and did not disrupt his sleep. He experienced no discomfort from the device, neither during dressing changes nor while the negative pressure was activated. As with most new technologies, there is a learning curve to applying the NPWT dressing and obtaining a seal that is minimal with relatively flat anatomical surfaces (eg, the pretibial area) but increases with anatomical curvature. The clinician needed 58 minutes to apply Mr. H’s initial dressing — he was one of the first patients we treated with this NPWT system. The time needed decreased to an average of 7 minutes (range 3–10 minutes) in subsequent applications.
Treatment. Mr. H was treated overnight in the ER with vancomycin HCl and piperacillin/tazobactam. His wound cultures grew light growth methicillin-sensitive Staphylococcus aureus (MSSA), rare growth Morganella morganii, and rare growth Bacteroides fragilis. One of two blood cultures done in the ER were positive for B. fragilis. An MRI was performed that revealed a small focal osteomyelitis at the distal tuft of the distal phalanx of the hallux. An aggressive excisional bedside debridement of the ulcer and bone was performed with a #15 blade scalpel, forceps, and rongeur in the ER. The remaining bone was firm to touch. After debridement, the ulcer measured 13 mm x 10 mm x 21 mm (length x width x depth) and probed to the distal phalanx of the hallux. Mr. H was discharged from the ER to home with wet-to-moist packing strip dressing changes three times a day and oral levofloxacin (500 mg) daily. He was further instructed to be nonweightbearing. Nine days after his initial presentation into the ER, Mr. H was seen for follow-up at the wound care center. His ulcer post-debridement measured 8 mm x 9 mm x 20 mm (length x width x depth) and continued to probe to firm bone (see Figure 1). He was started on the portable, nonelectrically powered NPWT system, continued on levofloxacin, and allowed to be weight-bearing in a postoperative shoe with a crest pad under the hallux and second toe to offload the ulcer (see Figure 2). The NPWT placement technique is described in Figure 3 and Table 1. After 4 weeks of treatment with the NPWT device, the oral antibiotic was discontinued per recommendation of an infectious disease consult. At week 5 (see Figure 4), NPWT was discontinued due to the small size of wound and Apligraf (Organogenesis, Canton, MA) was applied, followed by Mepitel nonadherent dressing (Mölnlycke, Switzerland) and Contreet foam (Coloplast, Denmark). Mr. H continued to use a postoperative shoe and crest pad. At follow-up 1 week post-Apligraf application, the ulcer was completely epithelialized. Mr. H was followed for an additional 2 months at increasing intervals and the ulcer remained healed (see Figure 5). Prognosis. Mr. H was extremely satisfied with the NPWT treatment. He reported the device did not interfere with his normal daily activities, was never noticed in social situations, and did not disrupt his sleep. He experienced no discomfort from the device, neither during dressing changes nor while the negative pressure was activated. As with most new technologies, there is a learning curve to applying the NPWT dressing and obtaining a seal that is minimal with relatively flat anatomical surfaces (eg, the pretibial area) but increases with anatomical curvature. The clinician needed 58 minutes to apply Mr. H’s initial dressing — he was one of the first patients we treated with this NPWT system. The time needed decreased to an average of 7 minutes (range 3–10 minutes) in subsequent applications.
Discussion
Diabetic ulcers occur on the toes usually related to trauma, footwear issues, and nail pathologies.12 In neuropathic feet, these ulcers often go unnoticed and can quickly probe to bone. Topical treatments not packed into the wounds commonly will result in superficial closure without granulation deep in the ulcer. In our experience, this closure can result in deep infection, perhaps because bacteria are enclosed. When this occurs, the ulcer may worsen and aggressive treatment must be initiated. These ulcers require excisional debridement, including infected bone. If the damage from infection is severe enough, amputation may be necessary; however, in our experience amputation often can be avoided through aggressive debridement. Soft, necrotic bone is removed through the ulcer using appropriate instrumentation until a good healthy bleeding base is left and hard bone is palpated. At this point, the standard of care for bone infection is 4 to 6 weeks of appropriate systemic antibiotic therapy, guided by bone culture results. If bone is not involved, soft tissue infections are typically treated with antibiotics for ~2 weeks. Decisions relating to advanced wound care are rendered by the treating practitioner.13 The most basic wound care for deep, small diameter ulcers consists of wet-to-moist packing with packing strips soaked in normal saline changed multiple times per day. In our experience, this can be very labor-intensive for patients and caregivers. Other options for packing include calcium alginate strips, which are removed and repacked every 1 to 3 days. Calcium alginate works well in heavily draining ulcers, but in our experience often can dry out an ulcer that needs a moist environment. Advanced therapies involving bioengineered dressings and skin substitutes also can be applied deep into the wound if no infection exists; however, it is difficult to apply a single layer in small-diameter ulcers without folding the skin substitute on top of itself. In our past experience, NPWT typically would have been avoided in these types of ulcers. The ability to get a seal with a stiff conduit is challenging when the toe is involved; once the seal is obtained, it is difficult to maintain when the toe moves. If the seal is obtained and maintained, the next challenge is for a patient to carry the negative pressure device, which leads from a toe up to a bag they must carry around. This is by no means impossible, but it is cumbersome for patients, particularly if they work or have balance issues. The new alternative NPWT device is designed for small diameter (<1.5 cm) deep toe ulcers. The gauze dressing allows packing into the deep ulcers. The integrated hydrocolloid increases the ability to conform the dressing around the port to the curved surface of the toe. The elasticity of the hydrocolloid also allows the toe to move and the dressing to give with movement, hence preventing leaks. It should be noted that due to circumferential placement of the hydrocolloid dressing around a toe and elastic recoil of the dressing, the dressing must be carefully applied so as not to form a tourniquet and strangulate the extremity or cause friction ulcers on adjacent toes. Once a seal is obtained, the tubing, which is integrated into the dressing, is cut to the desired length and connected into the cartridge that can be snapped into a strap attached to the lower leg. This allows the patient to ambulate without the constraint of a cumbersome device and to carry on activities with some semblance of normalcy.
Conclusion
NPWT has an important role in the treatment of DFUs. In our experience, it is a preferred method of treating ulcers that probe to or have exposed bone. Electric-powered negative pressure therapy devices on the market are reported to increase granulation tissue, decrease bacterial load, and cover exposed tendon and bone in larger ulcers, but have certain limitations relevant to smaller ulcers commonly seen in our clinics. The gauze and hydrocolloid dressing combination of the nonelectric NPWT system allows for packing into deep but small-diameter ulcers and facilitates use on ulcers typically deemed unsuitable for this modality due to the ulcer location or size. This system can help minimize the impact of NPWT on daily activities and provides a convenient, practical way to deliver NPWT.
References
1. Wu SC, Armstrong DG. Clinical outcome of diabetic foot ulcers treated with negative pressure wound therapy and the transition from acute care to home care. Int Wound J. 2008;5 (suppl 2):10–16. 2. Blume PA, Walters J, Payne W, Ayala J, Lantis J. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care. 2008;31(4):631–636. 3. Armstrong DG, Lavery LA. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet. 2005;366(9498):1704–1710. 4. Eginton MT, Brown KR, Seabrook GR, Towne JB, Cambria RA. A prospective randomized evaluation of negative-pressure wound dressings for diabetic foot wounds. Ann Vasc Surg. 2003;17(6):645–649. 5. Xie X, McGregor M, Dendukuri N. The clinical effectiveness of negative pressure wound therapy: a systematic review. J Wound Care. 2010;19(11):490–495. 6. Murdoch DP, Armstrong DG, Dacus JB, Laughlin TJ, Morgan CB, Lavery LA. The natural history of great toe amputations. J Foot Ankle Surg. 1997;36(3):204–208; discussion 256. 7. Armstrong DG, Marston WA, Reyzelman AM, Kirsner RS. Comparison of negative pressure wound therapy with an ultraportable mechanically powered device vs. traditional electrically powered device for the treatment of chronic lower extremity ulcers: a multicenter randomized-controlled trial. Wound Repair Regen. 2011;19(2):173–180. 8. Lerman B, Oldenbrook L, Eichstadt SL, Ryu J, Fong KD, Schubart PJ. Evaluation of chronic wound treatment with the SNaP wound care system versus modern dressing protocols. Plast Reconstr Surg. 2010;126(4):1253–1261. 9. Lerman B, Oldenbrook L, Ryu J, Fong KD, Schubart PJ. The SNaP Wound Care System: a case series using a novel ultraportable negative pressure wound therapy device for the treatment of diabetic lower extremity wounds. J Diabetes Sci Technol. 2010;4(4):825–830. 10. Hutton DW, Sheehan P. Comparative effectiveness of the SNaP Wound Care System. Int Wound J. 2011;8(2):196–205. 11. Fong KD, Hu D, Eichststadt BS, et al. Initial clinical experience using a novel ultraportable negative pressure wound therapy device. WOUNDS. 2010;22 (9):230–236. 12. Armstrong DG, Lavery LA. Diabetic foot ulcers: prevention, diagnosis and classification. Am Fam Phys. 1998;57(6):1325–1328. 13. Frykberg RG, Zgonis T, Armstrong DG, et al. Diabetic foot disorders. A clinical practice guideline (2006 revision). J Foot Ankle Surg. 2006;45(5 suppl):S1–S66.
This article was not subject to the Ostomy Wound Management peer-review process.
SaveSave




